Subcutaneous or intravenous rituximab? The SABRINA study
Immunochemotherapy induction followed by maintenance with rituximab is the current standard of care for patients with advanced-stage symptomatic follicular lymphoma. However, the fact rituximab has to be administered intravenously means the treatment is time (and costs) consuming. Recently, a new subcutaneous formulation of rituximab (RSC) has been developed which offers reduced treatment burden for patients compared to intravenous rituximab (RIV) as well as resource savings at the treatment facility. Additionally, availability of RSC would potentially allow patients to be treated primarily intravenously-free with orally administered partner therapies.
The phase 3 SABRINA study investigated induction RIV or RSC plus chemotherapy followed by maintenance RIV or RSC in patients with follicular lymphoma. Pharmacokinetic non-inferiority was previously reported for RSC (1400mg) compared with RIV (375mg/m2) as well as comparable efficacy and safety.1,2 At ASH 2016 Andrew Davies presented updated efficacy and safety results including overall response rates (ORR) at the end of maintenance and time to event (progression-free [PFS], overall [OS], and event-free [EFS] survival) data from the SABRINA study with a median follow-up of 37 months.
In this study 410 patients with treatment-naïve CD20+ grade 1–3a follicular lymphoma were randomized to receive RIV or RSC, stratified by FL International Prognostic Index score, chemotherapy regimen, and region. All patients received RIV 375mg/m2 in Cycle 1; for Cycles 2–8, patients received RIV 375mg/m2 or RSC 1400mg every 3 weeks. Patients received ≤8 cycles of CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) or 8 cycles of CVP (cyclophosphamide, vincristine and prednisone). During maintenance, patients received RIV or RSC every 8 weeks for 2 years. Non-serious adverse events were reported for 28 days following the last dose of rituximab. Serious adverse events were recorded for 1 year post-treatment or until the start of new anti-lymphoma treatment. Serious adverse events considered possibly related to study treatment were recorded indefinitely.
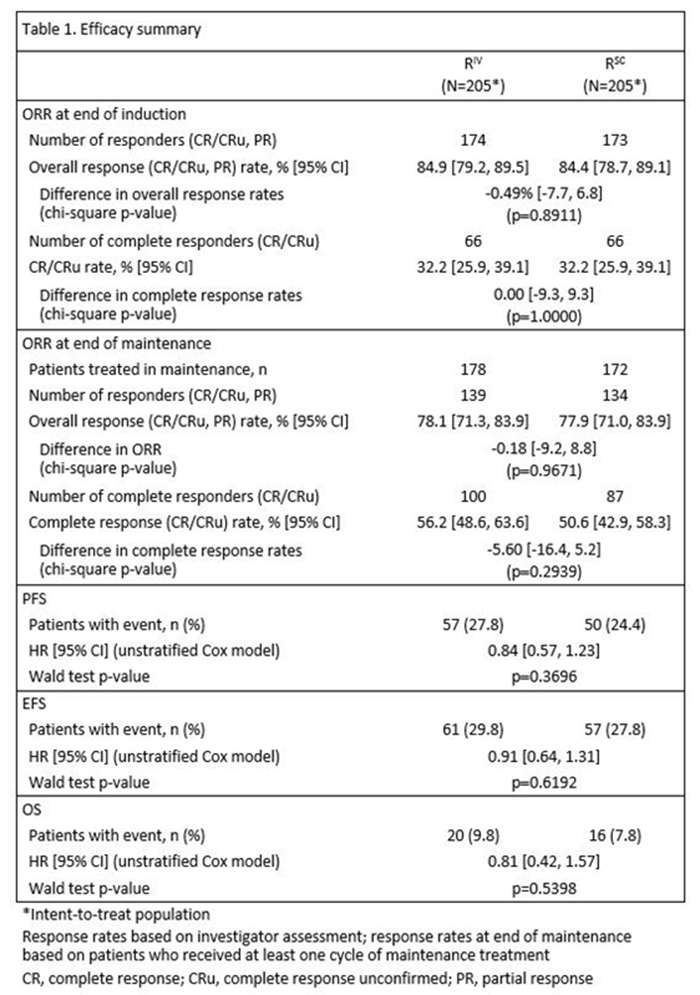
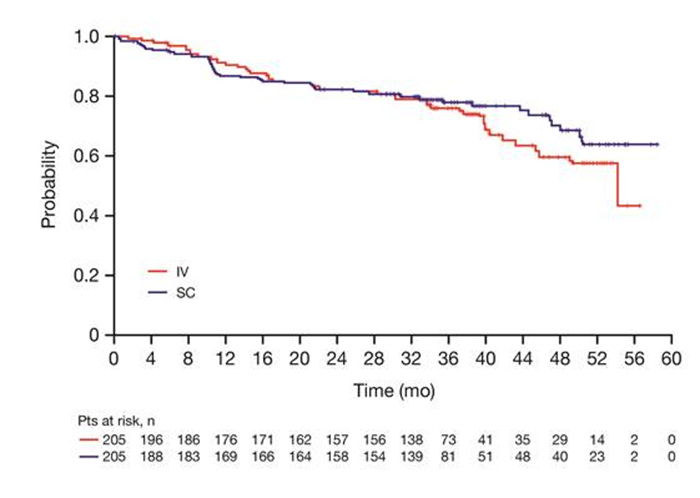
Based on investigator assessments for the intent-to-treat population (RIV n=205; RSC n=205), overall response rate at the end of maintenance was comparable between treatment arms: (78.1%, 95% CI [71.3, 83.9] for RIV versus 77.9%, 95% CI [71.0, 83.9] for RSC) (Table 1). Analyses of the time-to-event endpoints progression-free survival (HR, 0.84, 95% CI [0.57, 1.23]), event-free survival (HR, 0.91, 95% CI [0.64, 1.31), and overall survival (HR, 0.81, 95% CI [0.42, 1.57) showed no differences in efficacy for the subcutaneous versus the intravenous formulation. (Figure 1)
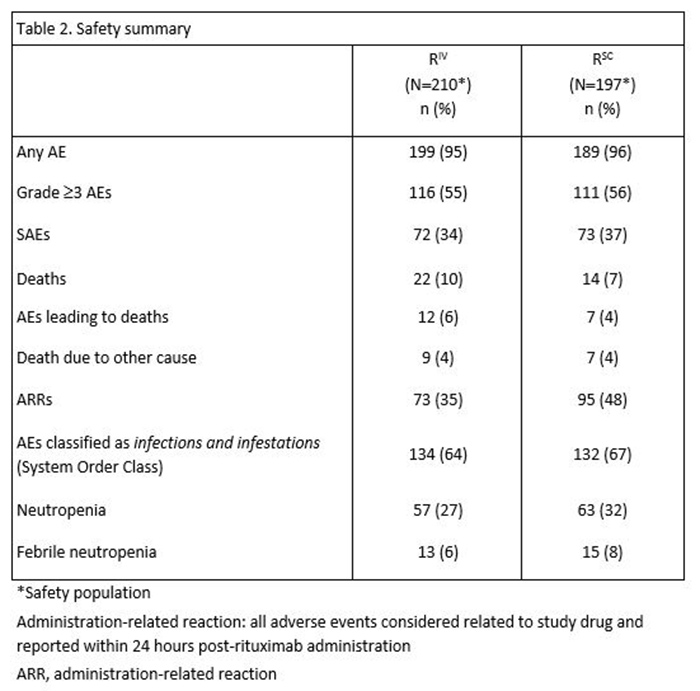
In total, 407 patients received ≥1 dose of rituximab (safety population). Six RSC patients discontinued treatment after Cycle 1 (RIV in both arms) and were included in the RIV safety population (RIV n=210; RSC n=197); 86% of patients started maintenance (RIV n=178, 85%; RSC n=172, 87%). Overall, there were similar incidences of patients with ≥1 adverse events (95% vs. 96%), grade ≥3 adverse events (55% and 56%), and serious adverse events (34% and 37%) for RIV versus RSC, respectively (Table 2). The most frequent adverse events reported overall (RIV vs. RSC) were neutropenia (27% versus 32%), nausea (22% versus 31%), constipation (26% versus 25%), cough (13% versus 23%), and fatigue (18% versus 20%). The most frequently reported adverse events during the maintenance phase of the study were upper respiratory tract infection (7% versus 11%) and cough (11% versus 12%) for RIV versus RSC, respectively. Overall, adverse events associated with B-cell depletion, including neutropenia, febrile neutropenia, and grade ≥3 infections, were balanced between the subcutaneous and intravenous treatment arms. The change in route of administration led to an expected higher incidence of local cutaneous reactions in the RSC arm (2% RIV versus 23% RSC) with injection site erythema, injection site pain, and rash being most frequently reported. All reported events, except for 1 adverse event of injection site rash in the RSC arm at Cycle 2, were of mild or moderate intensity (grade ≤2). Incidence of local cutaneous reactions decreased over subsequent treatment cycles. At data cut-off, 36 deaths had been reported: 20 (9.8%) in the RIV arm and 16 (7.8%) in the RSC arm.
In summary, this update of the SABRINA study showed no new clinically relevant safety signals observed with RSC and the safety profile was comparable to that of RIV. Response rates as well as progression-free and overall survival data for subcutaneous rituximab were comparable to intravenous rituximab and indicate that the anti-lymphoma activity of rituximab is not impaired when given subcutaneously. The availability of RSC administration over approximately 6 minutes has positive implications for patient and healthcare professional convenience, as well as healthcare resource savings, without compromising efficacy or safety.
Reference
Davies AJ, et al. Pharmacokinetics and safety of subcutaneous rituximab in follicular lymphoma (SABRINA): stage 1 analysis of a randomised phase 3 study. Lancet Oncol 2014;15:343–52.